Attention Deficit Hyperactivity Disorder (ADHD) is one of the most prevalent neurodevelopmental conditions affecting children and adolescents worldwide — with an estimated prevalence of 7.6% in children aged 3 to 12, and 5.6% in teenagers aged 12 to 18 (Sayal et al., 2018). Yet for decades, the clinical model of ADHD was built almost exclusively on research conducted with boys. This foundational bias has had profound consequences: girls have been systematically underdiagnosed, misdiagnosed, and left without appropriate support, sometimes until well into adulthood.
The differences between ADHD in girls and boys are not cosmetic or statistical. They reflect genuinely distinct patterns of symptom expression, developmental trajectory, comorbidity burden, and long-term functional impact. A 2024 systematic review synthesizing 67 studies confirmed that ADHD manifests differently across sexes in seven key domains: core symptoms, executive function, neuropsychomotor development, psychopathology, behavioral presentation, social functioning, and self-esteem (Tritto et al., 2024).
“Girls are not less impaired by ADHD than boys. They are differently impaired — and more systematically missed.”
— Tritto et al., Frontiers in Psychiatry, 2024This article provides a comprehensive, evidence-based overview of how ADHD presents differently in girls versus boys across childhood and adolescence, with dedicated attention to teenage boys — a population whose symptoms evolve significantly during puberty and are frequently misread as conduct problems, laziness, or defiance rather than recognized as neurodevelopmental struggle.
Core Symptom Differences: Girls vs. Boys
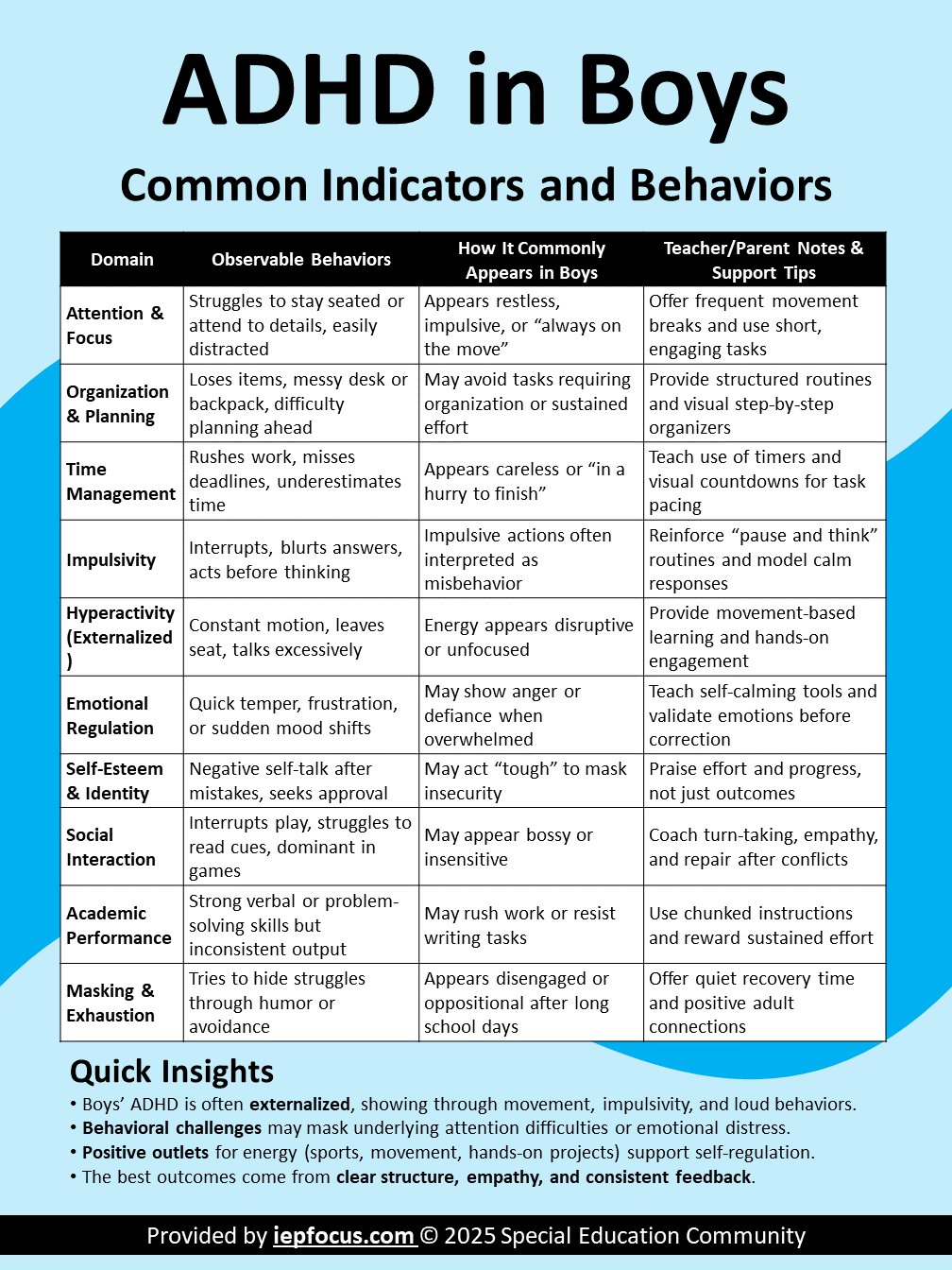
The most persistent clinical finding across decades of ADHD research is the externalizing vs. internalizing split. Boys with ADHD tend to externalize: they run, interrupt, act out, break rules. Girls with ADHD tend to internalize: they daydream, ruminate, mask their struggles, and develop anxiety and low self-esteem. These contrasting expressions stem from the same underlying neurobiology but produce radically different behavioral profiles.
| Domain | Boys with ADHD | Girls with ADHD |
|---|---|---|
| Primary symptom type | Hyperactive-impulsive; combined type predominates | Inattentive type predominates; internalized presentation |
| Hyperactivity expression | Physical: running, climbing, inability to sit still | Subtle: restlessness, fidgeting, excessive talking, nail-biting |
| Impulsivity | Overt: interrupting, rule-breaking, aggression | Covert: over-talking, social manipulation, risk-taking |
| Attention pattern | Broadly distracted; highly visible to teachers | Selective focus; daydreaming not immediately flagged |
| Emotional dysregulation | Explosive outbursts, reactive anger | Mood swings, emotional sensitivity, shame-based responses |
| Social behavior | Disruptive; conflict with peers; oppositional tendency | Social anxiety; people-pleasing; relational aggression |
| Academic visibility | Disruptive enough to trigger referral | Quiet underperformance; often attributed to effort or anxiety |
| Age of diagnosis | Earlier (childhood) | Later (adolescence or adulthood) |
The 2024 PRISMA systematic review (Tritto et al.) confirmed that while direct comparisons between diagnosed boys and girls sometimes show similar scores, the intra-sex effect of ADHD — how much it deviates from neurotypical peers of the same gender — is consistently larger in females. Girls are not less impaired; they are differently impaired, and more systematically missed.
The Externalizing vs. Internalizing Framework
Boys with ADHD show more co-existing externalizing disorders — conduct disorder and oppositional defiant disorder (ODD) — including aggression and rule-breaking behaviors. This visible disruption accelerates referral and diagnosis. Girls, by contrast, present more internalizing disorders, particularly anxiety, which often leads clinicians to treat the anxiety as the primary diagnosis while missing the underlying ADHD (Biederman et al., 2010; Hinshaw et al., 2012).
This misattribution is not trivial: anxiety symptoms can actually be more reliable identifiers of ADHD in girls than the behavioral diagnostic criteria themselves — a finding that underscores how profoundly current diagnostic frameworks were designed around male presentation (Skogli et al., 2013).
Girls with ADHD are more likely to receive anxiety or depression diagnoses before ADHD is ever considered. By the time ADHD is correctly identified, many have accumulated years of academic underachievement, fractured self-esteem, and untreated executive dysfunction.
ADHD in Teenage Boys: Symptom Manifestation in Adolescence
Adolescence transforms ADHD. The brain’s frontal lobe — the region governing impulse control, planning, and executive function — continues developing until approximately age 25. In teens with ADHD, this development is measurably delayed, creating a period of heightened vulnerability precisely when academic demands increase, social complexity peaks, and independence is actively sought (Wilens, 2024).
For teenage boys with ADHD, the shift is not simply that symptoms persist — it is that their expression changes in ways that can be misread as deliberate defiance, laziness, or personality problems rather than recognized as neurological struggles. The NIMH (2024) confirms that adolescents with ADHD typically show less overt hyperactivity and more restlessness, while inattention and impulsivity continue and increasingly affect academic performance, peer relationships, and risk behavior.
What Does ADHD Look Like in Teenage Boys?
Significant frontal lobe growth occurs between ages 12 and 25. In teen boys with ADHD, this development is delayed, meaning impulse control, conflict resolution, and long-term planning capacities mature more slowly than in neurotypical peers. This is a neurodevelopmental timeline difference — not a character flaw — and families and educators must account for it explicitly.
Greatest Risks Facing Teenage Boys with ADHD
Research consistently identifies four high-stakes risk areas for teenage boys with ADHD, all driven by the interaction of impulsivity, delayed frontal lobe maturation, and the independence demands of adolescence (Wilens, 2024; ADDitude Magazine, 2025):
How Do You Know if Your Boy Has ADHD?
Parents often wonder whether what they observe is typical teenage behavior or something more. The key distinction is not the presence of symptoms but their pervasiveness, persistence, and functional impact. ADHD must be present in at least two settings, must have begun before age 12, and must cause measurable impairment (DSM-5).
| Typical Teen Behavior | ADHD in Teen Boys |
|---|---|
| Occasional homework avoidance | Chronic inability to initiate most non-preferred tasks |
| Being distracted in class sometimes | Sustained inattention across most subjects, most days |
| Arguing with parents occasionally | Explosive, frequent conflicts; rapid escalation; poor repair |
| Energetic or restless after school | Cannot regulate movement or internal restlessness across all settings |
| Risk-taking as experimentation | Repeated impulsive decisions with limited awareness of consequences |
| Mood swings during stress | Emotional dysregulation that is disproportionate and chronic |
If you observe at least 6 symptoms of inattention or hyperactivity-impulsivity that have been present for more than 6 months, appear in multiple settings (home and school), and cause clear functional impairment — a formal evaluation by a pediatric psychologist or psychiatrist is warranted. Early identification dramatically improves long-term outcomes.
Marcus, Age 14 — Grade 9, ADHD Combined Type
- Profile
- Diagnosed at age 8, currently unmedicated after refusing treatment at 13. Flagged for disruptive behavior in three classes.
- Situation
- Frequently argues with teachers when assignments are returned, refuses to start written tasks, recently suspended for a physical altercation. Grades dropped from Bs to Ds. Parents report he games until 2am and “can’t be motivated.”
- Strategies
- Short, chunked written tasks with immediate feedback; behavioral agreement replacing punitive suspensions with structured re-engagement; family coaching on sleep hygiene; referral for medication re-evaluation; daily check-in with one trusted staff member.
ADHD in Teenage Girls: The Hidden Struggle
While boys’ ADHD often becomes more visible during adolescence, girls’ ADHD frequently becomes more hidden. As social demands escalate and academic expectations intensify, girls with ADHD deploy increasing cognitive effort to mask symptoms, maintain social appearances, and avoid the stigma of being seen as “not trying hard enough.” This compensatory masking is exhausting and unsustainable.
Hormonal changes during puberty directly impact dopamine regulation — a core mechanism in ADHD — meaning that girls may experience worsening symptom severity precisely as they face more complex social and academic environments. Research by Hinshaw et al. (2023) highlights that the majority of girls with ADHD will develop at least one significant comorbidity by early adulthood, with anxiety and depression being the most prevalent.
Nadia, Age 16 — Grade 10, Undiagnosed ADHD Inattentive Type
- Profile
- Referred by school counselor for “anxiety and declining academic performance.” Described by teachers as “bright but inconsistent.”
- Situation
- Receives high marks on discussions and oral presentations but fails to submit written assignments. Cries frequently, reports feeling “stupid,” and has recently withdrawn from her friend group. Her mother attributes it to teenage stress.
- Strategies
- Comprehensive psychoeducational assessment revealing ADHD as primary diagnosis. Extended time, assignment flexibility, and oral alternatives implemented. Weekly check-in with counselor framed around strengths. Parent psychoeducation on the female ADHD profile.
Diagnosis Gaps and Clinical Bias
The male-to-female ratio in clinical ADHD populations is approximately 3:1 in children and as high as 10:1 in some clinic-referred samples. Yet community-based epidemiological studies consistently report a ratio closer to 2:1 or 3:1 (Biederman et al., 2002). This discrepancy is not biological — it reflects systematic referral bias.
| Bias Source | Impact on Boys | Impact on Girls |
|---|---|---|
| Diagnostic criteria design | Criteria based on male behavioral profiles | Female presentations fall below threshold |
| Teacher referral behavior | Disruptive behavior triggers referral faster | Quiet inattention rarely triggers referral |
| Parent perception | Parents report hyperactivity/impulsivity readily | Parents may underestimate impairment in compliant girls |
| Clinician assumptions | ADHD expected; recognized efficiently | Anxiety/depression diagnosed first |
| Compensation capacity | Less likely to mask symptoms effectively | Girls more likely to mask, delaying detection |
| Diagnostic thresholds | Lower referral threshold | Higher threshold required before diagnosis is considered |
One proposed model suggests females require a greater genetic and environmental “load” to manifest ADHD at a level that triggers clinical diagnosis — implying that girls who are diagnosed are, on average, more severely impaired than diagnosed boys. The girls who are missed represent a large population of moderately affected individuals who receive no support at all (Eriksson et al., 2016).
Comorbidities by Gender
According to CDC data from a 2022 national survey, approximately 78% of children with ADHD have at least one co-occurring condition. The nature of those comorbidities differs significantly by gender — and understanding these patterns is critical for accurate differential diagnosis.
| Comorbidity | Boys with ADHD | Girls with ADHD |
|---|---|---|
| Anxiety disorders | 40% prevalence; often secondary to behavioral consequences | Often primary presentation; may mask ADHD entirely |
| Depression | Present; often secondary to academic failure | Higher risk; earlier onset; greater severity; associated with self-harm |
| ODD / Conduct Disorder | Significantly elevated; major referral driver | Less common; when present, appears later and less severely |
| Learning disabilities | Elevated prevalence | Less likely to co-occur than in boys |
| Substance use disorder | Elevated risk especially when unmedicated | Elevated risk post-puberty; self-medication pattern |
| Eating disorders | Lower prevalence | Significantly elevated in adolescence |
| Sleep disorders | Insomnia; delayed sleep phase common | Racing thoughts-driven insomnia; emotional dysregulation worsens sleep |
Undiagnosed girls with ADHD carry significantly elevated risk for major depressive disorder (with earlier onset and greater severity), self-harm behaviors, eating disorders, and unplanned pregnancy compared to neurotypical girls. These risks persist even after controlling for IQ, medication use, and age at diagnosis (Hinshaw et al., 2023).
Classroom Strategies for Boys and Girls with ADHD
Effective ADHD support must account for the distinct presentations in boys and girls. Strategies appropriate for the externalized, hyperactive profile of many boys may fail to address the internalized, compensatory profile of many girls — and vice versa.
For Boys with ADHD — Especially in Adolescence
For Girls with ADHD — Especially Inattentive Profile
Additional Case Studies
Jordan, Age 17 — Grade 11, ADHD Hyperactive-Impulsive Type
- Profile
- History of academic failure and two substance use incidents. Suspended twice in Grade 10 for cannabis possession and now on a behavior contract.
- Situation
- Significant difficulty completing independent work, frequently disrupts class by making jokes, and is at risk of not graduating. Teachers describe him as “charming but impossible.” Classroom disruption functions as escape from task demands.
- Strategies
- Functional Behavior Assessment (FBA) and BIP with positive replacement behaviors. Individualized graduation plan via project-based learning. Regular collaboration between trusted English teacher and behavioral team.
Amira, Age 13 — Grade 7, Newly Diagnosed ADHD Inattentive Type
- Profile
- Referred for anxiety and school refusal. Initially diagnosed with generalized anxiety disorder. Teachers describe her as “polite, quiet, and usually fine.”
- Situation
- Excels at verbal tasks; submits fewer than half of written assignments. Began refusing school in October citing stomachaches. Academic performance inconsistent but not flagged until school refusal escalated.
- Strategies
- Updated evaluation identifying ADHD Inattentive Type as primary diagnosis. IEP with extended time and check-in/check-out system. Gradual re-entry plan. Homework load reduced by 40% during reintegration. Family psychoeducation reframing refusal as executive overwhelm, not manipulation.
Frequently Asked Questions
These questions reflect real searches from parents, educators, and clinicians. Each answer is grounded in peer-reviewed research.
In teenage boys, ADHD often shifts away from obvious physical hyperactivity toward a more complex cluster of executive dysfunction, emotional volatility, and impulsive risk-taking. Rather than running around a classroom, a teen boy with ADHD may be chronically late submitting assignments, explosive when frustrated, unable to start tasks despite understanding them, and drawn to high-stimulation activities.
Impulsivity — now less supervised than in childhood — translates into reckless driving, substance experimentation, and social conflicts. Many teen boys with ADHD are described as “underperforming their potential.” This phrase misses the neurological reality: the executive systems required for independent academic work are genuinely impaired, not merely unexercised.
The NIMH (2024) confirms that adolescents with ADHD typically show less overt hyperactivity and more restlessness, while inattention and impulsivity continue to cause significant functional impairment across academic, family, and social domains.
Look for a persistent pattern (at least 6 months) of at least six symptoms of inattention or hyperactivity-impulsivity that appear in two or more settings (home and school) and cause measurable functional impairment. Key signs include: chronic difficulty completing tasks, forgetting assignments or materials, explosive emotional reactions, extreme restlessness, interrupting others, and repeated impulsive risk-taking.
The key is distinguishing typical teenage behavior from ADHD: ADHD symptoms are pervasive, persistent, and functionally impairing across multiple contexts — not situational or occasional.
A formal evaluation by a pediatric psychologist or psychiatrist is required for diagnosis. Do not rely on a brief checklist alone. Comprehensive assessments include parent and teacher rating scales, clinical interviews, and often cognitive testing to rule out other contributing factors.
ADHD can be diagnosed at any age, as long as symptoms were present before age 12. Clinically, the average diagnosis for children with obvious hyperactivity falls between ages 5 and 9. Children with the inattentive subtype — more common in girls and in intellectually capable children who compensate effectively — are frequently not identified until middle school, high school, or university.
A 2025 retrospective cohort study of 144,103 patients found a significant increase in adult ADHD diagnoses after 2020, reflecting a generation of individuals missed during childhood (Paul et al., 2025). Late diagnosis, while better than no diagnosis, is associated with greater cumulative academic and psychological harm — particularly for girls whose symptoms were less visible to teachers and parents.
There is no upper age limit for ADHD diagnosis. Adults routinely benefit from identification and appropriate support even when diagnosed for the first time in their 30s, 40s, or beyond.
Chez les garçons adolescents, le TDAH prend souvent une forme différente de celle observée dans l’enfance. L’hyperactivité physique diminue généralement, remplacée par une agitation interne, une procrastination chronique, des explosions émotionnelles, et une prise de risques impulsive.
Sur le plan scolaire, le garçon peut sembler capable mais incapable de terminer ses travaux, d’organiser son temps, ou de démarrer une tâche sans aide. Les comportements risqués augmentent à l’adolescence : conduite imprudente, expérimentation de substances, conflits sociaux.
Ces manifestations sont souvent interprétées à tort comme de la paresse, de l’insolence, ou un problème de caractère. Ce sont en réalité des expressions de la dysfonction exécutive liée au TDAH, exacerbée par le développement neurologique encore incomplet du lobe frontal durant l’adolescence. La maturation du lobe frontal se poursuit jusqu’à environ 25 ans, ce qui explique pourquoi les adolescents avec un TDAH ont un contrôle inhibitoire significativement plus faible que leurs pairs.
Les signes à observer incluent : difficulté persistante à maintenir l’attention, oublis fréquents, incapacité à finir les tâches, agitation constante, impulsivité (interrompre les conversations, prendre des décisions sans réflexion), et dysrégulation émotionnelle disproportionnée.
Ces comportements doivent être présents depuis au moins six mois, dans au moins deux contextes différents (maison et école), et doivent causer une gêne fonctionnelle réelle. Il est important de distinguer le TDAH des comportements adolescents typiques : la fréquence, la persistance, et l’impact sur la vie quotidienne sont les indicateurs clés.
Une évaluation formelle par un neuropédiatre, un psychologue, ou un psychiatre est nécessaire pour poser un diagnostic. Ne pas attendre que la situation s’aggrave : une identification précoce améliore considérablement les trajectoires scolaires et émotionnelles à long terme.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). APA Publishing.
- Biederman, J., Mick, E., Faraone, S. V., et al. (2002). Influence of gender on ADHD in children referred to a psychiatric clinic. American Journal of Psychiatry, 159(1), 36–42.
- Centers for Disease Control and Prevention. (2024). Data and statistics on ADHD. cdc.gov
- Eriksson, M., et al. (2016). Female protective effect in ADHD: Replication and extension. Journal of Child Psychology and Psychiatry, 57(5), 557–563.
- Gilbert, M., et al. (2025). Gender and age differences in ADHD symptoms in the BELLA Study. Child Psychiatry and Human Development, 56, 1162–1172.
- Hinshaw, S. P., et al. (2023). Another inconvenient truth: Race and ethnicity in ADHD treatment research. Journal of Consulting and Clinical Psychology, 91(6), 541–553.
- Mowlem, F., et al. (2019). Sex differences in predicting ADHD clinical diagnosis and treatment. European Child and Adolescent Psychiatry, 28(4), 481–489.
- National Institute of Mental Health (NIMH). (2024). Attention-deficit/hyperactivity disorder: What you need to know. NIH Publication No. 24-MH-8300.
- Paul, M. L., et al. (2025). Incidence of ADHD between 2016 and 2023: A retrospective cohort. Psychiatric Research and Clinical Practice, 7(1), 18–24.
- Sayal, K., et al. (2018). ADHD in children and young people: Prevalence, care pathways. The Lancet Psychiatry, 5(2), 175–186.
- Shaw, P., et al. (2020). Adolescent ADHD: Understanding teenage symptom trajectories. British Journal of Psychiatry, 217(3), 579–588.
- Skogli, E. W., et al. (2013). ADHD in girls and boys: Gender differences in co-existing symptoms. BMC Psychiatry, 13, 298.
- Tritto, A., et al. (2024). Sex differences in children and adolescents with ADHD: A literature review. Frontiers in Psychiatry. PMC12222223
- Wilens, T. E. (2024). ADHD in teens: Challenges and solutions. ADDitude Magazine.
- Zetterqvist, V., et al. (2025). Adolescents’ experiences of living with ADHD — a thematic analysis. BMC Psychology, 13, 75.
{kind=link}